A New Weapon Against Polio - A modified vaccine offers hope that eradication is closer than ever - BY JASON KEYSER
In mid-2017, two groups of 15 strangers lived together for 28 days each in a ring of shipping containers assembled in the parking lot of Antwerp University Hospital in Belgium. They had access to books and movies, a small courtyard for barbecues, a common kitchen and dining room, and a fitness room — all of it behind secure interlocking doors and under the watch of personnel in protective gowns.
What sounds like a reality TV or sci-fi scenario was, in fact, a remarkable clinical trial of the latest weapon in the battle to eradicate polio — a reengineered vaccine called the novel oral polio vaccine type 2, or nOPV2......
The study aimed to evaluate whether the altered formula, the first major update to polio vaccines in about six decades, could help end outbreaks of circulating vaccine-derived poliovirus, also known as variant poliovirus. Such cases arise in rare instances when the live but weakened virus contained in oral polio vaccines circulates in areas of low vaccine coverage and mutates back into a dangerous form that can infect people who have not been fully vaccinated.
These variant poliovirus outbreaks have emerged over the past two decades as a significant stumbling block in the effort by Rotary and its partners in the Global Polio Eradication Initiative (GPEI) to wipe out the disease. The outbreaks are different from those driven by wild poliovirus, which circulated naturally in the environment for millennia and remains endemic in just two countries, Afghanistan and Pakistan. But the outcome is the same — the virus in either kind of outbreak can, in rare instances, cause paralysis.
In 2011, staff at the Bill & Melinda Gates Foundation, one of the GPEI partners, wondered if the live virus in the traditional oral vaccine could be tweaked to limit its ability to mutate. "The first challenge was purely scientific," says Ananda Bandyopadhyay, a deputy director of the polio team at the Gates Foundation, which funded and led the effort. "How do you make the vaccine more genetically stable without compromising its immunogenicity [ability to provoke an immune response]? That was really, really challenging."
Even then, researchers would need to figure out how to test the idea. Any attempt would require strict isolation of study participants. At a 2015 meeting in Brussels, Bandyopadhyay pitched the audacious idea to Pierre Van Damme, director of the Centre for Evaluation of Vaccination at the University of Antwerp. "We had to be very creative," says Ilse De Coster, who would lead the clinical trial team with Van Damme in Belgium, "because at that time we didn’t have any facility that was developed for containment."
They considered sequestering study participants at isolated holiday resorts or vacant centers that had been used to house asylum seekers, eventually settling on the idea of a purpose-built modular container village, dubbed Poliopolis by Van Damme’s wife. The center’s scientists had conducted more than 500 vaccine trials but had little experience with polio, which long ago ceased to be of daily concern in the country thanks to routine immunization.

Viewable Image - purpose built container village in antwerp
Image Caption
At Poliopolis, a purpose-built container village in Antwerp, Belgium, nOPV2 vaccine trial participants had to live together for 28 days, sealed off from the outside world. "It was surreal," says Caro Bouten, a volunteer from the Netherlands whose aunt had polio. PHOTOGRAPH: UNIVERSITY OF ANTWERPFor much of the developed world, polio is a distant memory. Long gone are the days of the summertime terrors in Europe and North America in the 1940s and 1950s when children went to bed with what their parents thought was a mild flu only to wake up rubber-limbed and burning with fever. Thousands were paralyzed. Some ended up in the dreaded iron lung device that enclosed the body up to the neck and helped them breathe.
There is no cure for polio, but with the development of vaccines in the 1950s and subsequent routine immunization, the United States and Belgium saw their last wild polio cases in 1979. Vaccination campaigns went global in the decades that followed, with Rotary launching PolioPlus in 1985 and helping found the GPEI in 1988. The goal was to eradicate a human disease for only the second time in history, after the World Health Organization declared the world free of smallpox in 1980.
In 1988, wild poliovirus paralyzed hundreds of children every day, with an estimated 350,000 polio cases across more than 125 countries that year. Since then, cases have plummeted 99.9 percent, sparing an estimated 20 million children from paralysis. From January to early August of this year, 14 cases of wild polio were confirmed in Pakistan and one in Afghanistan — the last two countries where it is consistently present. Four additional cases were reported in Mozambique in an outbreak that began in Malawi in late 2021 and was linked to a virus strain that had circulated in Pakistan.
That progress would not have been possible without the oral polio vaccine. "It’s a critically important tool and has saved millions of lives and prevented paralysis," Bandyopadhyay says.
A vaccine developed in the early 1950s by virologist Jonas Salk using killed virus, known as the inactivated polio vaccine, or IPV, carries no risk of seeding vaccine-derived, or variant, outbreaks, because the killed virus cannot mutate. Many places use this vaccine, which is injected, for routine childhood immunization. But it only protects the vaccinated individual and cannot prevent person-to-person spread, which is required in an eradication program.
The oral polio vaccine, or OPV, was developed in the late 1950s by physician Albert Sabin. It’s become the vaccine of choice for polio eradication because it’s safe, inexpensive, and easy to administer, and the live but weakened vaccine virus replicates in the gut and produces strong intestinal immunity. As a result, vaccinated children can shed the weakened vaccine virus in their stool for several weeks. In areas with poor sanitation, the weakened virus spreads, stimulating an immune response in the unvaccinated.
But this ability of the weakened virus to circulate carries a vulnerability in areas of low immunity — one that stayed hidden for years, until 2000.
When children started getting sick that year in the Dominican Republic and neighboring Haiti, no one suspected the cause was polio, which hadn’t been seen in the Americas for nearly a decade. Initially, pesticide poisoning was blamed.
From July 2000 to July 2001, 21 children were paralyzed on the island shared by the two countries. Two of them died. A virologist from the U.S. Centers for Disease Control and Prevention analyzed stool samples from two paralyzed children and found that the cause was, in fact, polio.
More troubling was where precisely the virus came from. This was not wild polio. The weakened vaccine virus had circulated unchecked for too long and had mutated and become virulent. Researchers had long speculated such a scenario was possible, but until then it had never been detected.
All but one of the children in the Caribbean outbreak were either unvaccinated or incompletely vaccinated, researchers found. They were from communities with vaccination rates as low as 7 percent. "It’s not really a vaccine issue; it’s a vaccination issue," Bandyopadhyay says of the variant outbreaks. "It only evolves if there is a population where we are not immunizing properly and not all the susceptible kids are getting the vaccine."
Some 3.2 million children were quickly vaccinated on the island, and the outbreak was stopped. But the risk of variant poliovirus outbreaks became clear, along with the need to improve vaccination rates in vulnerable communities everywhere.
Most variant cases involve type 2 poliovirus, one of two strains that have been eradicated in the wild. In 2016, the year after its eradication was certified, the type 2 strain was removed from oral vaccine formulas, in part, to avoid the risk of seeding new vaccine variant outbreaks during routine immunization campaigns. It seemed like the right moment to make the change, which was recommended by the Strategic Advisory Group of Experts on Immunization, an independent body advising WHO. There were only two reported type 2 vaccine variant cases that year, one in Pakistan and the other in Nigeria. But virus modelers at the time underestimated the amount of type 2 vaccine variant poliovirus still circulating around the world.
The number of children paralyzed by the type 2 variant poliovirus surged from two in 2016 to more than 1,000 at its peak in 2020, spread over two dozen countries, most of them in Africa. The situation was made worse by a four-month halt to immunization campaigns during the COVID-19 pandemic that left 80 million children unprotected. "It created a window for further expansion of the outbreaks," says John Vertefeuille, chief of the polio eradication branch at the CDC. Variant cases now vastly outnumber cases of wild polio, though they are starting to decline.
The existing oral polio vaccine containing only type 2 virus — reserved for outbreak response since the 2016 formula switch — has been effective in stopping most variant poliovirus outbreaks. But still, that vaccine carries the risk of the virus mutating back to a more virulent form if it circulates in populations with low immunity. At the Gates Foundation, there was a realization that a new type 2 oral polio vaccine was needed, and fast. "This entire situation with the variant poliovirus outbreaks is a challenge, but it’s also an opportunity to innovate," Bandyopadhyay says.
The foundation established and funded a scientific consortium to develop the new oral vaccine, including the UK’s National Institute for Biological Standards and Control and the University of California San Francisco. Researchers at those two institutions altered part of the old type 2 vaccine virus’s genome to make it more genetically stable while preserving its ability to produce strong immunity in the gut. But the challenge of how to test it in humans without risking environmental spread remained.

Viewable Image - a polio vaccination team visits a home in karachi
Image Caption
A polio vaccination team visits a home in Karachi, Pakistan, in August. More than 60 percent of vaccine workers in the country are women, helping to build trust and convince mothers to vaccinate their children. PHOTOGRAPH (OPPOSITE): KHAULA JAMIL
Viewable Image - poliopolis was constructed in just three days
Image Caption
Poliopolis was constructed in just three days. To the researchers’ knowledge, no one had ever attempted a containment study quite like it. Volunteers had to undergo medical and psychological screenings to ensure they were up to the challenge and could function as a group. PHOTOGRAPH: UNIVERSITY OF ANTWERPThe team at Poliopolis was moving fast. The 66 containers, which were prefabricated off-site, were assembled in just three days in April 2017 and were ready for operation a month after that. Altogether, it had been less than half a year since the team decided to proceed with the Poliopolis concept. To the researchers’ knowledge, no one had ever attempted a containment study in such a purpose-built facility and for so long.
Other vaccine trials requiring containment measures have been carried out in hospitals and even motels. But since vaccinated people shed the weakened virus from the oral polio vaccine in their stool for several weeks, researchers would need a facility where sewage could be strictly contained, kept separate from public waste systems, and decontaminated. Clothing, towels, utensils, uneaten food, and anything else handled by participants would be disposed of securely or decontaminated with chlorine dioxide gas. Entrances were interlocking, meaning an inner door could not open until an outer one locked.
Because of the length of time the virus can continue to be excreted, trial participants would have to stay sequestered for at least 28 days. Volunteers had to undergo medical and psychological screening to ensure they were up to the challenge and could function as a group. "We had two psychologists who screened the subjects," says De Coster, adding that participants had access to mental health support throughout the trial. "They talked a lot about possible scenarios that could happen with your family while you are inside and how will you cope with that. What are you going to do if one of your children at home will become ill, for instance? The subject is a volunteer, so that means they always can quit the study. But this time there was a lot at stake."

Viewable Image - a polio vaccinator marks a child
Image Caption
A polio vaccinator marks a child’s pinkie after vaccinating him outside a home in Karachi, Pakistan. By early August of this year, 14 cases of wild polio were confirmed in Pakistan and one in neighboring Afghanistan — the last two countries where wild poliovirus is endemic. PHOTOGRAPH (OPPOSITE): KHAULA JAMILVolunteers, most from neighboring Netherlands, included a housewife, a student finishing a master’s thesis, and a working professional who wanted a little time off. They got along well despite occasional friction over insignificant things like messes in the kitchen. "Put some people together and there will be friction, like on the reality TV show Big Brother," explains Caro Bouten, one of the volunteers. "I was writing a book, so I didn’t care. I’d go back to my room. I had a focus. So that helped me."
Polio left Bouten’s aunt with a limp, a leg brace, and a difficult life at a boarding school, separated from a family that felt ashamed of the condition. Those memories, along with her work as a nurse and counselor for refugees, motivated her to join the study. She realized just how important it was afterward when she was invited to meet the queen of Belgium.
The trial was conducted with two back-to-back groups of 15 volunteers from May to August in 2017. (Only one volunteer left early, on the evening before the final day, though he returned the next day to complete remaining study requirements.) Further studies were conducted on adults in Belgium and children and infants in Panama. NOPV2 received the first emergency use listing for a vaccine by WHO in November 2020. The vaccine was rolled out in March 2021, first in Nigeria and Liberia. Through the first half of 2022, more than 370 million doses were administered in more than 20 countries.
"It’s looking very promising, and it’s looking like it’s doing what it is supposed to do: induce population immunity and interrupt transmission in most settings and with a much lower risk of seeding new outbreaks," Bandyopadhyay says. "It’s that data that gives me the confidence that this is one of those tools that could be the turning point."
The new vaccine, by itself, is not a silver bullet. It won’t stop transmission if immunization campaigns cannot reach close to 90 percent of children in the response zones. Adding to the challenge in Africa, a drop in routine childhood immunizations during the COVID-19 pandemic has led to surges in cases of measles, yellow fever, cholera, and other infectious diseases, leaving governments with other public health priorities. "It’s hard for polio to always be top of the list," says WHO’s Simona Zipursky, co-chair of the nOPV2 working group, which includes all GPEI partners. "That’s where we have really benefited from the partnership, and Rotarians have played a really key role in that advocacy."
Integrating polio response with other important community needs is key to gaining trust and cooperation, she says. That’s crucial because underimmunization remains an obstacle, allowing cases of variant polio to leap across the globe and pop up in places where the disease hasn’t been seen in years. Officials detected polio in London and New York City sewage this year, for instance. And in July 2022, health authorities announced an unvaccinated man in New York state had been sickened with variant poliovirus genetically linked to the spread in London.
We’ve never been closer than we are now has been a frequent refrain for the polio eradication campaign, but there are plenty of reasons to believe it today. The global community is united around the latest GPEI strategy. The Taliban leadership that returned to power in Afghanistan a year ago agreed to allow house-to-house immunization campaigns to resume nationwide after a 3 ½-year ban in some areas, raising hopes that the remaining reservoirs of wild polio can soon be extinguished. And there are more scientific innovations in the pipeline, including more genetically stable versions of the oral vaccines for the other two types of polio, modeled on nOPV2.
Like many polio campaigners, Nana Yaa Siriboe, a member of the Rotary Club of Accra Labone, Ghana, has a personal stake in crossing the finish line. Her cousin is a survivor who once needed crutches but now walks unaided, with only a limp. "My mother would tell her, ‘I’m not going to allow you to think that you’re going to be helpless,’" she recalls. "And I tell you, my cousin is a fighter."
Siriboe became chair of the Ghana PolioPlus Committee in 2019, just as variant polio cases were emerging in the country, about a decade after it was declared polio-free. She mobilized Rotary volunteers to visit homes, schools, mosques, churches, and markets to find and immunize children, and the outbreaks were suppressed for two years. But polio paralyzed one person this June, prompting another mass immunization campaign that was to start in August.
The arrival of nOPV2 gives her hope. So do the mothers she has watched over the years bringing their children to be vaccinated. "It’s a joy," she says of meeting the children. "You get to play with them. Some like to see their little finger marked with the pen to show this child has been immunized. We give them toffee. It’s a wonderful experience."
Help leverage the opportunity to reach a polio-free world. Make your contribution at endpolio.org/donate.
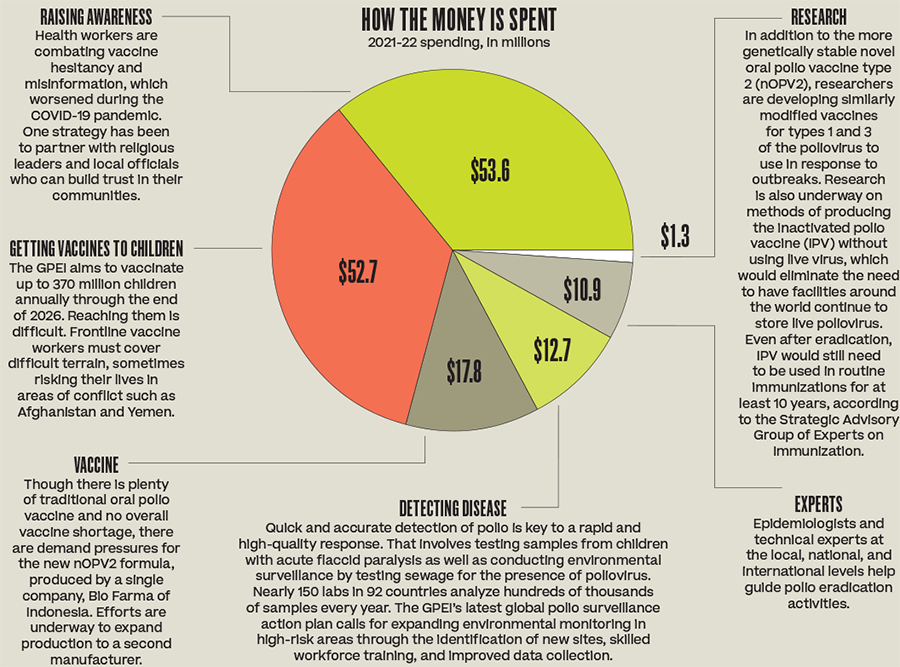
The global health community has the knowledge and tools to extinguish polio. When it will deliver on that promise depends largely on funding for everything from reaching children with vaccines to battling misinformation. The last mile of the journey, as campaigners point out, is the toughest. • In April, the Global Polio Eradication Initiative launched an appeal for $4.8 billion to fund its 2022-26 strategy for speeding up outbreak response times, making vaccination campaigns more effective, and gaining access to hard-to-reach areas. Germany is co-hosting a pledging event for the GPEI strategy at the World Health Summit in Berlin in October. • A fundraising partnership between Rotary and the Bill & Melinda Gates Foundation generates up to $150 million each year to contribute to the effort. Here is a look at how that money is used: